Authors: Joep Kraeima, Femke Schröder, Tim Boers, Maaike Koenrades, Simeon Ruiter, Maarten van Alphen, Anna Ooms, Roel Verhoeven, Jasper Smit and Frank Halfwerk
Domain of image-guided interventions
The domain of image-guided interventions envelops advanced imaging diagnostics and monitoring, data-driven artificial intelligence supported surgical interventions and 3D-planning, visualisation and per-operative surgical navigation. As a result, technical physicians apply and develop these technological innovations in surgical domains as cardio-thoracic, colorectal, general (oncological), neuro, orthopaedic, oral and maxillofacial, paediatric, plastic, and vascular surgery, as well as interventional radiology, medical oncology, and pulmonology.
Surgical skills are mastered in a mandatory Technical Medicine Master course up to a proficiency level in simulation-based setting before students enter their clinical rotations [1]. It’s redesign at the University of Twente in 2021 involved 10 clinical cases from technical physicians throughout the Netherlands and from the aforementioned domains. It was the first time NVvTG-experts in surgery and interventions met for their joint expertise, and a need for clustering was defined. At the same time, the Netherlands Society for Surgery (NVvH) asked for participation of NVvTG members in their national Surgical Innovations Working Group. Thus, NVvTG cluster innovative surgery and interventions was instigated early 2022 by the NVvTG member council, and is now known under its current name “NVvTG cluster image-guided interventions”.
The aim of this cluster is to allow patients throughout the Netherlands the highest level of image-guided interventions provided by technical physicians, quality assurance of technical medical practice including medical device regulation application, and cluster knowledge and skill transfer and development. This cluster members is well-represented in the Dutch Healthcare Disciplinary Board (Regionaal tuchtcollege) to ensure medical practice standards for individual patient care.
Technological developments are implemented faster in society than in medicine, and result in an ever growing mismatch in clinical practice [2]. For image-guided interventions, technical physicians accelerate innovations in direct patient care in hospitals, and address their clinical need to industry, while industry employed technical physicians target groups of patients and direct research and development into relevant solutions for actual (technical) medical problems.
Form technical medical doctor to cluster expertise
The cluster of image-guided interventions has expertise in several core domains, where technical physicians align, improve, and provide specialized technical medical care for patients.
3D technology, virtual surgical planning and computer assisted surgery
A technical physician can specialize in the field of 3D technology, virtual surgical planning and computer assisted surgery. Those technical physicians, who are members of the cluster image-guided interventions, work for medical 3D labs and/or a related clinical departments, such as Oral and Maxillofacial Surgery, Orthopaedics, Trauma- and Neurosurgery, Cardio-Thoracic Surgery which have integrated 3D technology in their standard of care.
A medical 3D lab is a specialized facility within a hospital that develops, validates and implements innovative diagnostics and treatment optimisation using 3D printing and other image-based technologies such as fluoroscopy and virtual reality. These medical 3D labs are commonly EU-MDR compliant facilities that, as in-house medical device developer, may produce patient specific 3D printed anatomical models, surgical guides (PSG) and implants (PSI). Medical 3D labs initiate improved patient care by means of their activities in innovation, scientific research, and medical education within their respective hospitals. Medical 3D labs can be located within specific clinical departments or organized hospital-wide, similar to facilitating departments such as radiology, providing the entire hospital access to their medical 3D expertise. In the Netherlands, all academic centres and some teaching hospitals have established medical 3D labs.
Clinical Care
An essential aspect of medical 3D labs is adding information and context to the decision-making process. The technical physician advises or requests the most optimal imaging protocols and processes data acquired to a patient-specific treatment plan. Often the data is visualized in anatomical models, representing the patient specific anatomy, pathologies, or anatomical deviations. Those models provide valuable assistance during multidisciplinary meetings when making surgical plans or as an addition to patient communication counselling. In specific surgeries a translation to the operating theatre is made with 3D printed anatomical models, cutting guides, patient specific implants or surgical navigation.
An anatomical model is created based on CT or MRI scans, where relevant structures are segmented to generate a 3D mesh for 3D printing. When a preoperative plan is integrated into a virtual 3D model, it is referred to as a VSP. This planning can be applied for various pathologies and thereby medical specialties, such as oral and maxillofacial surgery, orthopaedic surgery, neurosurgery, or trauma surgery.
In cases where a patient-specific guide (PSG) is required for executing the VSP during surgery, technical physicians are mostly in the lead to develop the optimal guides. It is important that PSG precisely align with the patient's anatomy, ensuring optimal bone seating. Guides often contain saw slots and drill sleeves, allowing pre-cutting and pre-drilling to achieve the desired correction. In some cases, repositioning guides are used, eliminating the need for pre-drilled holes when the specific plate choice is uncertain. Instead, the repositioning guide is adjusted on the k-wires during the surgery to achieve the optimal planned position. Some centres also develop patient-specific implants for specific patient care, particularly in maxillofacial surgery & oncology application.
Scientific Research
Medical 3D labs are still relatively new in the medical field, leading to a considerable amount of research within these labs. Technical physicians are actively engaged in these innovation and scientific developments. Current examples include patient-specific reconstruction of the mandible as an oncology research line.
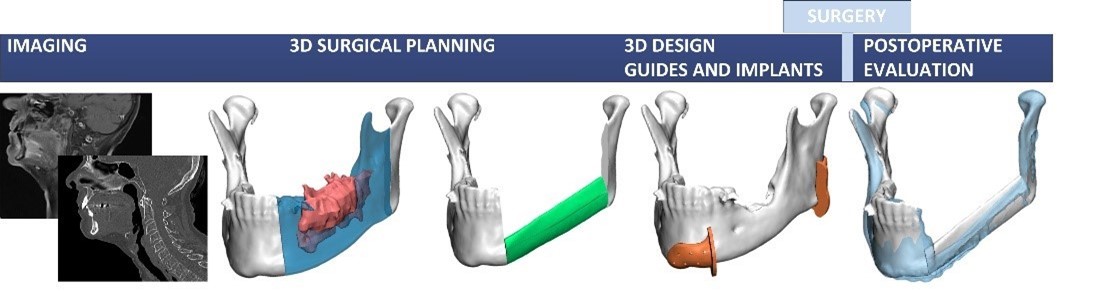
Surgical removal of squamous cell carcinomas in the oral cavity close to or within mandibular bone, often necessitates resecting part of the mandible with a microscopic free margin of at least 5 mm on both sides of the resection, according to current clinical guidelines. The oncological-surgical challenge is to plan and perform an adequate resection with sufficient margin, based on the pre-operative information. Nowadays, mandibular malignancy resections frequently include the use of 3D VSP and guided surgery techniques based on CT data. Both intra-operative navigation and 3D printed surgical guides have been proven to provide precise translation of the 3D VSP to the surgical procedure [4-6]. The planning for adequate tumour removal should include detailed bone information as well as tumour characteristics such as localisation, size, shape and extension. The combination of information with regard to localisation, extent, size and shape, as provided by CTs and MRIs is crucial for adequate resection planning [7]. A validated workflow was developed in the 3D lab of the University Medical Centre Groningen, which has now been standard of care and still is an active research line and state of the art in its field (see Figure 1).
{kind=link}
Figure 1 Schematic overview of workflow developed by a technical physician. This includes a method to combine both CT and MRI datasets for 3D visualisation of the bone (CT) and tumour (MRI). This method optimised 3D VSP for mandible malignancy resections. Clinical application led to an improvement of tumour free bone resections for 100% of the cases in this study [8]. This underlines the added value of a technical physician for creating a multi-modality, more complete, 3D model for 3D VSP.
IMAGE GUIDED DIAGNOSTICS AND THERAPEUTIC INTERVENTIONS
Historically, imaging technologies first came to visualize patients in a manner infeasible before. The stethoscope for example – already a piece of technology – was slowly supplied with X-ray imaging. With these imaging technologies, previously invisible information became apparent and could be used to determine a diagnostic or treatment plan in better detail. Not long after the introduction of such imaging devices, innovative physicians however also started using these technologies not only for observing patient and tissue function but also to help guide the interventional procedure to target the supposed affected area itself for tissue diagnostics or therapeutics. These imaging technologies are used to help visualize or analyse tissue structures intra-operatively such that the intervention with secondary device for diagnostics or therapeutics can take place in a less invasive manner, with improved precision, higher effectiveness and/or safety. The devices used along with imaging equipment for obtaining tissue or curing the patient of their pathology are generally specialistic of nature and developed towards keyhole access of patients.
The range of diagnostics and therapeutics in this field is ever increasing, as well as its complexity level. Depending on complexity, image-guided interventions can be widely adopted and implemented or is only available in specialized (tertiary referral) centres to ensure sufficient patient volume to obtain expertise.
Technical physicians specialized in the field of image-guided interventions occupy themselves with pathologies and care pathways where specific technical and medical expertise is needed to ensure accurate and safe diagnostics and therapy of patients. Two technical physician subspecialties can be defined that have been forming since the inception of this new profession: Interventional oncology and cardiovascular interventions. These specialties knowingly surpass conventional medical specialties such as the interventional radiology, surgery, cardiology and oncology departments where the majority of the more complex procedures in this field take place as the technical medical expertise needed for performing these procedures is overarching.
INTERVENTIONAL ONCOLOGY
Cancer is a leading cause of death worldwide, accounting for nearly 10 million deaths in 2020, or nearly one in six deaths [9]. It is one of major health impacts both from a patient and societal perspective. The goal of interventional oncology (IO) is to offer cancer patients a personalized treatment strategy of the least invasive but most accurate nature through imaging guidance of miniaturized diagnostic and therapeutic instruments. Type of IO procedures includes percutaneous biopsies, tumour ablation, trans arterial therapies and pain management. The technical physician in the field of interventional oncology incorporates the understanding of tumorigenesis and evolution with a technological understanding of technology systems to provide care in the best possible manner.
The workflow of IO procedures consists of planning, targeting, intervention, confirmation of intervention and follow-up. In every step of this workflow, image guidance is essential and can also consist of fusion of two or more imaging techniques such as CT, fluoroscopy, MRI, ultrasound and PET.
Depending on disease stage and patient care pathway, procedures focus on obtaining tissue diagnostics or a therapeutic effect. In all instances, this image guidance and fusion is a central focus of being able to reach the disease site. Lesions or (suspected) pathological tissue are accessed by rigid or flexible miniaturized instruments, depending on the availability of safely accessible pre-existent orifices leading to the region of interest and if instruments can be developed in such a way that they allow flexible or rigid miniaturization.
IMAGE GUIDED RIGID NAVIGATION AND THERAPEUTICS
The technical physician in interventional oncology utilizing rigid navigation to reach deeper situated organs generally does so under global imaging techniques such as MRI, CT or equivalent technologies. Local imaging techniques such as can be applied superficially (i.e. US, photo-acoustics, OCT) might also be utilized to guide secondary instruments. The target tissue herein is generally positioned such that a flexible approach to the tissue is infeasible because of navigation means, consequent limitations in therapy (i.e. microwave ablation of a tumour by a flexible device from within a vessel is considered infeasible) or the unavailability of structures that can guide flexible instruments to these locations.
Rigid video-endoscopy is not necessarily considered the (main) imaging instrument of choice in this field, as these would imply translations of conventional surgical approaches rather than interventional oncology interventions.
Image guided flexible navigation
The technical physician in interventional oncology utilizes flexible instruments to reach deeper situated organs. Complex patient anatomy which also mobilises with rigid or flexible navigation make these procedures challenging. Imaging such as MRI and CT is therefore routinely complemented with local imaging technologies such as intra-operative ultrasound, videoscopy or techniques in which pre- and intra-procedural imaging is manipulated and visualized such to the operator that it alleviates some of the difficulty in (3D) interpretation.
Upcoming domains and interaction with other clusters
The cluster of image-guided interventions provides expertise on e-health and peri- and post-operative monitoring for both vital signs and rehabilitation [12-14]. It is likely that these underdeveloped domains mature in the coming years and align with other clusters in technical medicine.
Technical physicians in MedTech industry
While the educational program of technical medicine was initially developed to train technical physicians for employment within hospitals, technical physicians have also entered career paths in medical technology industries. Not only are they present in already longer existing and larger MedTech companies, they also contribute to development of medical technology in smaller companies such as start-ups and scale-ups. Whether products are developed for (early) diagnosis, treatment in hospitals or monitoring of patients in their home environment, it is essential that the right choices are made during the first phases of development. Technical physicians contribute during product verification and validation processes to ensure successful clinical implementation.
Clinical experience obtained during their studies and subsequent doctoral and clinical trainings is pivotal for bringing technologies to hospitals. This technical-medical point of view accelerates initial product development and verification before the first clinical introduction. Understanding both technology and production steps help in a consulting and management role towards clinical users.
Technical physicians fulfil many roles in MedTech companies, e.g. as clinical scientist or medical engineer where product development of new surgical techniques or medical devices are performed. Technical physicians in industry often have direct relationships with the clinical end-users, and together aim to improve healthcare. Products as (patient-specific) medical tools, prosthetics, surgical guides, etc. for hospitals or other medical industries help to understand patient-specific anatomy, thus saving time and cost in the operating theatre.
Last, technical physicians contribute in the complex process of medical device regulation (MDR) interpretation by ensuring compliance. Technical-medical validation and quality assurance of medical products according to ISO 13485 bring technologies faster to patients.
Simulation-based training
Surgical skills should be trained before practice on patients, and therefore before clinical rotations in the hospital. This cluster is taking responsibility for the mandatory Master course Surgical Skills for Technical Medicine students at University of Twente.
Surgical patient route is cornerstone in the proficiency and simulation-based course [1], with pre-operative, per-operative and post-operative lectures, group meetings and wet lab sessions. Students have to pass a theoretical test, and technical skills assessment with scrubbing and donning, local anaesthesia, excision, and suturing before they can practice in patient care. Image-guided interventions cluster technical physicians are involved in state-of-the art clinical cases with challenging problems. Overall, this prepares students for their clinical rotations with proficiency in surgical skills and behaviour [1], and confidence to practice these skills [15].
Outlook
This chapter shows nationwide adoption of technical physicians in individual care with impact on global collective patient care. The dynamic discipline of technical medicine will grow in the coming years into a cornerstone of MedTech application and development.
How to measure success?
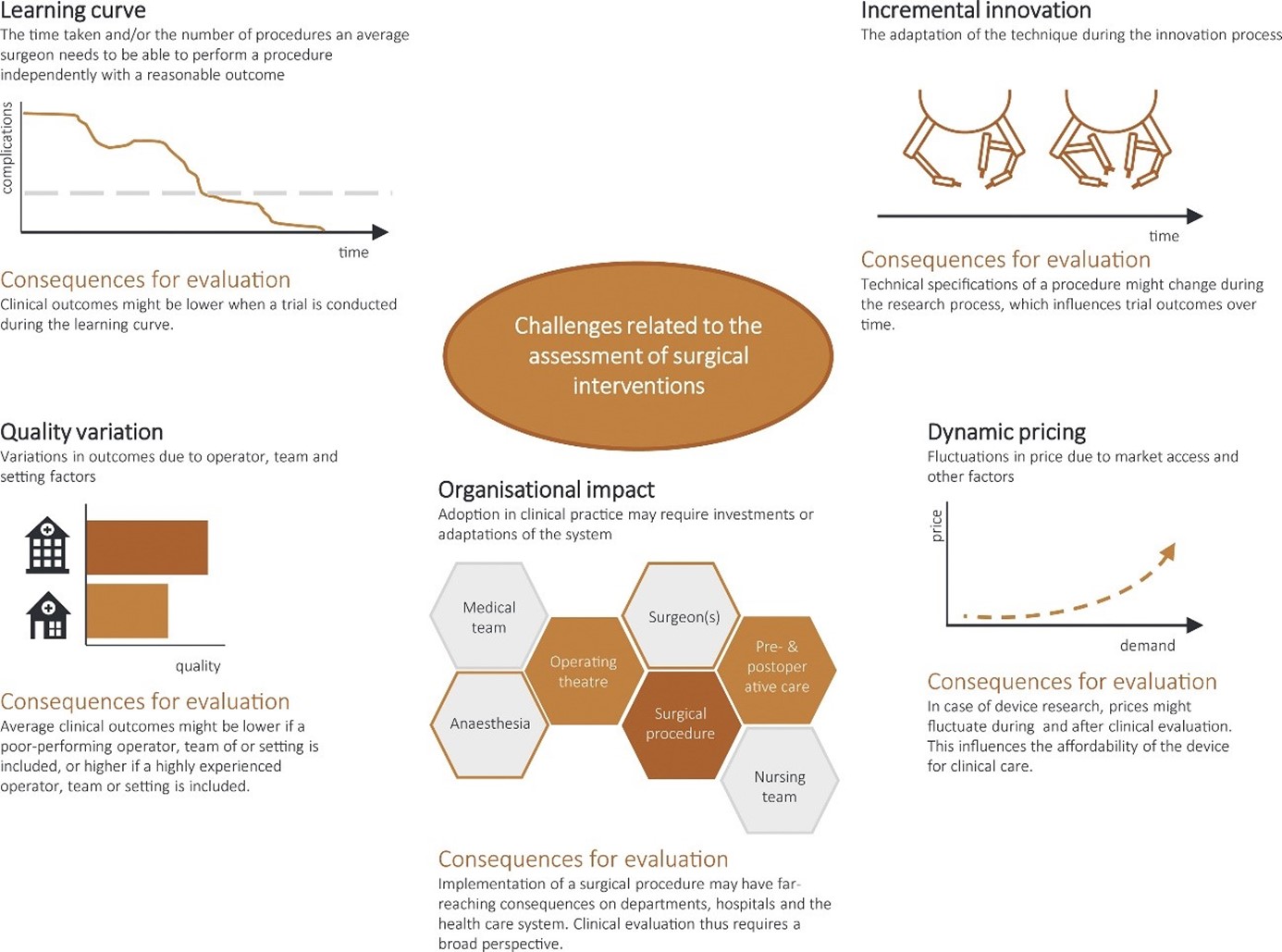
Inventarisation and evaluation of technological innovations is challenging [16]. When and how to measure impact is often unclear, with professionals and organisations still learning during early evaluation. Furthermore, adaptation of technology leads to incremental innovation, among other challenges for assessing surgical interventions (See Figure 2).
{kind=link}
Figure 2 Challenges and consequences for evaluating surgical interventions. Image from [16] under CC-BY license.
Outcomes of image-guided interventions should be defined and measured for each phase of adoption: from pre-clinical studies to first in humans, and from one specialist centre to general adoptation [16]. The IDEAL (Idea, Development, Exploration, Assessment, Long-term follow-up) framework [17] will help to determine the impact of this cluster to the field of surgery and interventions.
3D technology, virtual surgical planning and computer assisted surgery
Technical Physicians have proven to be essential for developments and improvements in surgical treatments using 3D technology. The high-tech health professional is the cornerstone of most 3D medical labs in the Netherlands. Since 3D technology has become widely available over the past years, 3D labs on one hand have a responsibility in routine care and guaranteeing their production towards clinicians and patients, and on the other hand need to look out for new developments and related technologies.
In the near future a reduced need for anatomical models is expected with a growing reliance on virtual visualization. As virtual reality (VR) and mixed reality technologies advance, these models may be entirely replaced by virtual simulations, eliminating the need for physical models. Haptic feedback and touch-and-feel need to be improved to fully replace physical models.
Additionally, improvements in computer software reduce the necessity for manual processing of 3D models. Virtual preoperative planning is anticipated to remain essential and become standard of practice for low-volume and high-complex surgery. Future planning is likely to become more automated or semi-automated, making it more scalable. As mixed reality techniques become more reliable, virtual planning could be visualized through VR headsets during surgery. It is expected that surgical robots will be used more frequently in the future. These robots will require a detailed preoperative plan for performing surgeries. Therefore, we anticipate that there will continue to be a role for technical physician to design this plan, both now and in the future.
Image guided diagnostics and therapeutic interventions
Historically, the therapeutic area of interventional oncology has been assumed a second best alternative or even a salvage therapy. Depending on organs and tissue involved, it is preferred only after surgical resection and possibly radiotherapy. With the advent of people becoming increasingly older and better treatment options, previously incurable disease is slowly becoming a chronic disease requiring repeat (local) intervention. The role of image guided interventions in interventional oncology is therewith becoming increasingly important. With further development of techniques, it might also progress into a first line of treatment rather than a second or third to surgery or radiotherapy.
Clinical pathway-ownership for technical physicians in the diagnosis, therapy and follow-up of thyroid nodule management are to be expected. Applying advanced imaging modalities such as 3D ultrasound thus improving the diagnosis by feeding these volume data to computer aided diagnosis software will aid individual patient care. Pre-operative nodule ablation planning with 3d-analyses help navigate ablation and allow for detailed follow-up. A technical physician can perform all these tasks, and such hyper-specialisation will reduce inter-observer variation and improve patient outcomes.
In cardiovascular interventions, the shift to using only image guided procedures to help these patients has – for the vast part – already been made. The image guided approach to treat these patients in a minimal invasive approach is now by default endovascular access. We envision that these developments continue to accelerate in the coming years.
Acknowledgements
The authors gratefully acknowledge editorial support from Jarah Kessler and Lysette Scheepmaker.
Disclaimer and potential conflicts of interest
All authors are technical physicians (technical medical doctors) in Dutch hospitals, academia or industry. NVvTG cluster image-guided interventions board members Femke Schröder, Roel Verhoeven, Simeon Ruiter and Frank Halfwerk were invited early 2023 to write this book chapter of Principles of Technical Medicine. Cluster members were subsequently invited to contribute and jointly wrote this book chapter.
Femke Schröder discloses financial contribution from In2Med to improve patient-specific guided sacroiliac joint fusion procedures and stocks in MedTech industry.
Tim Boers discloses a grant from Wetenschapsfonds ZGT for material expenses and research into thyroid nodules and a recent NVvTG board membership.
Frank Halfwerk discloses positions as associate scientific committee membership of SESAM (Society in Europe for Simulation Applied to Medicine), lecturer and course co-coordinator in surgical skills for technical medicine, expert-member technical physician in Dutch Healthcare Disciplinary Board (Regionaal Tuchtcollege ‘s Hertogenbosch), and ambassadorship of the ICARUS Global Surgical Collaboration Working Group, as well as receipt of DeltaScan devices, training, and reduced consumable fees for a clinical delirium study from Prolira.
Maarten van Alphen received an ATOS Medical research grant for laryngectomies care, and has a patent pending on additive manufactured heat and moisture exchange.
Roel Verhoeven discloses institutional and departmental research contracts with Pentax medical, AstraZeneca, Johnson & Johnson, Philips, Siemens Healthineers, Intuitive, Innovative Health Initiative, KWF, as well as consulting fees from Intuitive, Johnson & Johnson, NLC paid to the institution, travel support from Intuitive, Pentax medical and Johnson & Johnson, equipment gifts from Philips Medical, and a current board membership of NVvTG.
Simeon Ruiter received consulting fees from SIRTEX medical. AO works for Oceanz.
Joep Kraeima discloses SNN EFRO Funding Personalised implants and PPP allowance - research.
Maaike Koenrades has a patent pending on apatient-specific guide for minimal invasive procedures and reports institutional payment for educational activities for technical medicine.
Jasper Smit discloses to work for Bcon Medical and own stock appreciation rights, and received medical equipment from Philips for research in a previous employment.
References
[1] Halfwerk F, Groot Jebbink E, Groenier M. Development and Evaluation of a Proficiency-based and Simulation-based Surgical Skills Training for Technical Medicine Students. MedEdPublish 2020;9.
[2] Maassen H. ‘De kloof tussen geneeskunde en techniek is groot’. Medisch Contact. Utrecht: Koninklijke Nederlandsche Maatschappij tot bevordering der Geneeskunst (KNMG),. 2021:3.
[3] Schroder FF, de Graaff F, Vochteloo AJH. Patient-Specific Guided Osteotomy to Correct a Symptomatic Malunion of the Left Forearm. Children (Basel) 2021;8.
[4] Schepers RH, Kraeima J, Vissink A, Lahoda LU, Roodenburg JL, Reintsema H et al. Accuracy of secondary maxillofacial reconstruction with prefabricated fibula grafts using 3D planning and guided reconstruction. J Craniomaxillofac Surg 2016;44:392-9.
[5] Bittermann G, Scheifele C, Prokic V, Bhatt V, Henke M, Grosu AL et al. Description of a method: computer generated virtual model for accurate localisation of tumour margins, standardised resection, and planning of radiation treatment in head & neck cancer surgery. J Craniomaxillofac Surg 2013;41:279-81.
[6] Wilde F, Hanken H, Probst F, Schramm A, Heiland M, Cornelius CP. Multicenter study on the use of patient-specific CAD/CAM reconstruction plates for mandibular reconstruction. Int J Comput Assist Radiol Surg 2015;10:2035-51.
[7] Blatt S, Ziebart T, Kruger M, Pabst AM. Diagnosing oral squamous cell carcinoma: How much imaging do we really need? A review of the current literature. J Craniomaxillofac Surg 2016;44:538-49.
[8] Kraeima J, Dorgelo B, Gulbitti HA, Steenbakkers R, Schepman KP, Roodenburg JLN et al. Multi-modality 3D mandibular resection planning in head and neck cancer using CT and MRI data fusion: A clinical series. Oral Oncol 2018;81:22-28.
[9] Zhang J, Wu W, Ren Y, Yuan Y, Jia L. Electroacupuncture for the treatment of cancer pain: a systematic review and meta-analysis of randomized clinical trials. Front Pain Res (Lausanne) 2023;4:1186506.
[10] Tinguely P, Ruiter SJS, Engstrand J, de Haas RJ, Nilsson H, Candinas D et al. A prospective multicentre trial on survival after Microwave Ablation VErsus Resection for Resectable Colorectal liver metastases (MAVERRIC). Eur J Cancer 2023;187:65-76.
[11] Heerink WJ, Ruiter SJS, Pennings JP, Lansdorp B, Vliegenthart R, Oudkerk M et al. Robotic versus Freehand Needle Positioning in CT-guided Ablation of Liver Tumors: A Randomized Controlled Trial. Radiology 2019;290:826-32.
[12] Halfwerk FR, van Haaren JHL, Klaassen R, van Delden RW, Veltink PH, Grandjean JG. Objective Quantification of In-Hospital Patient Mobilization after Cardiac Surgery Using Accelerometers: Selection, Use, and Analysis. Sensors 2021;21:1979.
[13] Breteler MJM, Numan L, Ruurda JP, van Hillegersberg R, van der Horst S, Dohmen DAJ et al. Wireless Remote Home Monitoring of Vital Signs in Patients Discharged Early After Esophagectomy: Observational Feasibility Study. JMIR Perioper Med 2020;3:e21705.
[14] ten Dam L, Dijkstra K, Halfwerk FR. De QUALITY studie, effecten van eHealth op angstklachten en kwaliteit van leven van de postoperatieve cardiochirurgische patiënt. Cordiaal 2022;44:82-85.
[15] Halfwerk F, Groot Jebbink E, Groenier M. Proficient before practice - Graduate simulation-based surgical skills training increases confidence in technical skills. 27th Annual Meeting of Society for Simulation in Europe 2022. Seville, Spain, 2022.
[16] Scholte M, Rovers MM, Grutters JPC. The Use of Decision Analytic Modeling in the Evaluation of Surgical Innovations: A Scoping Review. Value in Health 2021;24:884-900.
[17] Hirst A, Philippou Y, Blazeby J, Campbell B, Campbell M, Feinberg J et al. No Surgical Innovation Without Evaluation: Evolution and Further Development of the IDEAL Framework and Recommendations. Annals of surgery 2019;269.